Delivery is the expulsion from the uterus of a mature offspring—a truly miraculous event in the creation of new life, one that has developed over centuries and has taken on several modes for the welfare of the woman and child.
Spontaneous, vacuum/forceps-assisted delivery, or CS has advantages and disadvantages, and anyone working with expectant parents must thoroughly understand all three.
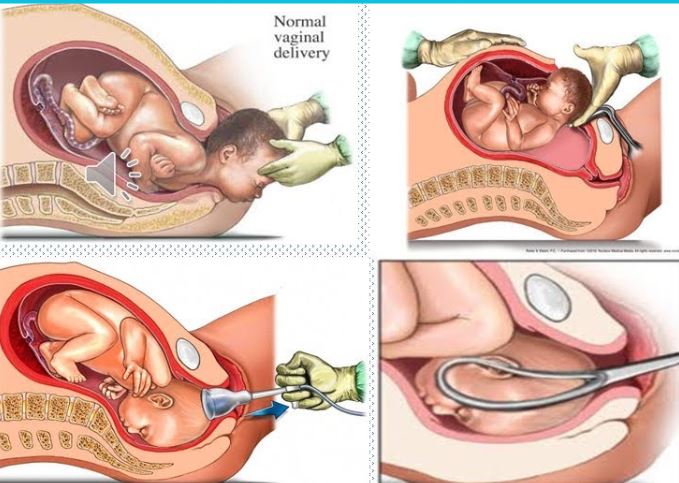
Spontaneous delivery
It is also known as vaginal birth, a process in which the baby is born through the vaginal canal without any medical operations. This method usually starts with the onset of labour, that is, the process described by rhythmic uterine contractions that cause cervical expansion and, in the end, allow the baby to move through the birth canal. Spontaneous delivery corresponds to natural labour patterns and provides hormonal and physiological advantages for both mother and baby. Compared to operative deliveries such as CS, mothers who deliver spontaneously often enjoy better, more rapid recovery intervals and shorter postpartum hospital stays. Additionally, the chance for immediate postnatal skin-to-skin contact, which is easily promoted following spontaneous delivery, stimulates the initial bonding process between mother and baby.
However, some of the possible complications of spontaneous vaginal delivery include severe and prolonged labour pains for some women, hence the need for pain management methods such as epidurals or analgesics. Additionally, there could be lacerations and tears in the vaginal or perineal region, hence the need for sutures. While spontaneous deliveries are considered generally safe, some of the events experienced during delivery, including foetal distress or prolonged labour, would need the intervention of medical professionals.
Vacuum/Forceps delivery
Vacuum extraction and forceps delivery are medical procedures for vaginal delivery of the neonate when either slow progress in labour or the well-being of either the mother or baby prompts concern. Vacuum extraction involves a suction cup attached to the baby’s head and is designed to assist in the baby’s delivery, whereas forceps are special instruments intended for holding the baby’s head and leading it through the birth canal.
Both these processes accelerate parturition in cases of progressive labour or when foetal distress is present, and the life of a baby can be saved from these procedures, which in a way rule out the need for a cesarean section with a more invasive procedure and very long recovery time. However, it is important to note that the application of either vacuum or forceps delivery also poses great risks of trauma—scarring the scalp and bruising the face or lacerating either the mother or the baby.
Improper application or excessive force during the delivery can result in complications such as skull fractures or even nerve damage. Also, it is critical to mention that vacuum and forceps deliveries cannot have universal application, especially in cases where the position of the infant is unfavourable, or when there are express contraindications in instrumental delivery.
Cesarean section
This medically common C-section is an operation where the segments are delivered through the mother’s uterus, which is made into the abdominal skin. C-sections may either be planned (elective) or carried out in emergency cases when complications arise during labour.
This allows a controlled and predictable delivery environment, thereby reducing risks to both mother and neonate, such as foetal distress, cephalopelvic disproportion, and birth injuries. Cesarean sections are delivery operations, so some common and significant inherent risks include infections, haemorrhage, and reactions to anaesthetic agents, and these procedures also take a much longer recovery time compared to a vaginal or vacuum/forceps delivery.
Moreover, several repeated cesarean sections can make a subsequent pregnancy riskier due to complications like uterine rupture and placenta previa.
Current trends and global data
Over the past decades, there has been a noticeable worldwide increase in cesarean section rates. The global average cesarean section rate increased decidedly from 12.1 per cent to 21.1 per cent over the 15 years from 2000 to 2015 based on WHO numbers, with region and country-specific differences being particularly worthy of note. While cesarean delivery is necessary in saving lives sometimes, in most cases, it just assumes a life of its own, and the increasing C-section rates have become a source of concern as the intensity of medicalisation of birth and unwarranted interventions increases.
On the other hand, there has been growing appreciation and support for vaginal birth; its adoption is measured in the work of reducing unnecessary cesarean deliveries and increasing access to supportive care during labour. Other techniques, like induction of labour and continuous support during labour – for example, with a doula and other methods of non-pharmacological pain control, have become recognised as measures toward the promotion of spontaneous vaginal deliveries and decreasing medical interventions.
However, vacuum and forceps deliveries remain highly pertinent to the practice of obstetrics; these procedures bridge a gap formed between spontaneous vaginal delivery and cesarean section. Most practitioners continue to appreciate the role played by these procedures in the current practice of obstetrics.
| Type of deliveries | 2080 Shrawan – 2081 Baisakh | 2079 Shrawan – 2080 Ashad | 2078 Shrawan – 2079 Ashad | 2077 Shrawan – 2078 Ashad | 2076 Shrawan – 2077 Ashad |
| Spontaneous | 1779 | 2141 | 2290 | 2964 | 3055 |
| Vacuum / Forceps | 49 | 50 | 89 | 184 | 84 |
| CS | 370 | 530 | 494 | 771 | 492 |
Source: Rapti Provincial Hospital
Maternal health care has improved in Nepal but it is still a challenge. In this regard, the need to consider local factors may have served to skew the observed in this data set.
One alarming trend is the drastic reduction in the number of spontaneous deliveries year after year. This again suggests that it could be in the close delineation of a decline in the number of health care services rendered in the prenatal stages either due to a loss of access or diminution in the quality of previously available services, resulting in constraints of the normalcy of pregnancy and hence fewer natural births. Factors in changing health demographics could be increasing maternal age or an increase in the incidence of non-communicable health conditions that complicate pregnancy. It should be further researched whether hospital policies are more and more oriented to interventions in the place of natural birth if it is not so medically needed.
The forceps and vacuum delivery numbers indicate different levels of differences before increasing. This might be due to a decrease in the availability of spontaneous delivery numbers, in which compensatory assisted delivery is reached in the process. The second cause would be differences in staff or resources; availability in the number of experienced professionals or equipment availability may also determine the number of assisted deliveries.
One interesting trend is that there is a marked decline in the number of Caesarean sections performed over this period. This reflects either a genuine willingness to pursue natural birth, wherever possible and supportable, resulting from strengthened awareness-raising campaigns or hospital policy changes. There is still a high possibility that surgical interventions have been restricted due to resource-related issues. Further research is needed to explore how trends in patients’ preferences for natural birth are evolving in the context of Nepal.
While thoroughly analysing the data presented above, irrespective of the types of deliveries, the total number of childbirths in Rapti Provincial Hospital has been reduced.