In the course of living, everyone goes through difficulties in life, which might be mental or physical challenges. Some have to deal with a physical disability, some have to deal with mental problems and there are a few who have to deal with different sexual identities.
Moreover, intersex is a biological condition where one is defined as a person born with a combination of male and female biological traits having different intersex conditions. Intersex refers to a group of conditions in which there is a discrepancy between the external genitals and the internal genitals.
Androgen insensitivity syndrome (AIS) is the most common cause of 46, XY intersex. Those with androgen insensitivity syndrome have to deal with both mental and physical challenges as they grow up. It is necessary for androgen insensitivity syndrome patients to understand their condition fully, and encourage doctors to treat them with empathy, not as a science experiment.
Understanding androgen insensitivity syndrome
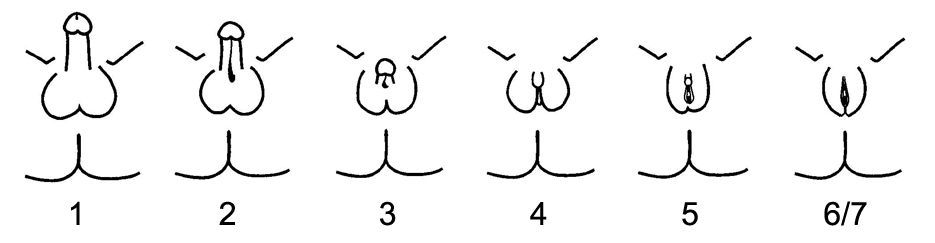
Androgen insensitivity syndrome is a spectrum that consists of three broad phenotypes: complete androgen insensitivity syndrome (CAIS), partial androgen insensitivity syndrome (PAIS), and mild androgen insensitivity syndrome (MAIS), depending on the amount of residual receptor function.
Standard references quote the prevalence of CAIS as 2:100,000–5:100,000. PAIS has a similar prevalence of 5:100,000–7:100,000. The prevalence of MAIS is yet to be determined.
‘Gender ambiguous’ and ‘hermaphrodite’ are some inaccurate terms used in the past to describe androgen insensitivity syndrome patients. The accepted norm in the 80s and 90s was not to tell children with androgen insensitivity syndrome their diagnosis, because they could get bullied for it, and it was assumed that if nobody knew about it or asked questions, then it was fine.
In 46, XY intersex, the person has the chromosomes of a male, but the external genitals are incompletely formed, ambiguous, or clearly female due to a defect in androgen action. So, they are genetically male and phenotypically female. To understand the mental and physical condition of a person with androgen insensitivity syndrome here is a real-life experience of a 40-year-lady (Intersex) with androgen insensitivity syndrome.
Her journey as an intersex
A 40-year-old lady (Intersex) with androgen insensitivity syndrome states that growing up in a small town was difficult as she tried to figure out why she was different from other girls of her age.
This lady was diagnosed with androgen insensitivity syndrome at the age of 15 years and did not fully know her diagnosis until she was 26 years old. As a 15-year-old, she was —a little awkward, super ADHD, probably a little bit autistic, definitely very neurodivergent, and going through a lot.
She had never got her period like her friends did, and she was constantly terrified that she was suddenly going to get her period at school. Around this time, she got ill with a stomach parasite, and an abdominal ultrasound was ordered, which revealed a mass. The doctors said that the mass was likely the reason she had not had her period and was referred to a gynaecology doctor.
At the hospital, she had her first pelvic examination done without explaining anything to her. She says, ‘‘They put me in this tiny room. God, I can smell it, so bad. I can see it in my mind…they wouldn’t let my mother be in the room and the doctor inserted three fingers in my vagina and pressed the abdomen, and said: “It feels like everything is there”. The doctor left, and then I wiped my blood off the table, I put on the clothes, and cried”.
The doctor said the reason she had not started her period was psychosomatic. He said, ‘‘She was clearly having a sexual identity crisis, some kind of feelings about becoming a woman. If she lost some weight, ran some laps at school, wore some frilly dresses, grew out her hair, and painted her nails, she would get her period.
He added the scan was unclear and they were “making something out of nothing’’. This visit was an emotionally distressing experience. Her mother even filed some complaints, but nothing was done.
The second opinion
They got a second opinion. During this appointment, she told them she did not want to be touched but was open to answering questions and having a conversation. Nobody was explaining anything to her, all the discussions were with her mother. The doctor did not do a pelvic exam. The doctor said she thought she knew what was wrong and referred her to an endocrinologist.
At 15, she was only told she had a risk for cancer and her gonads had to be removed. She was also told she had a lot of scar tissue and was physically incapable of intercourse until it was corrected surgically, which was not true.
Her mother was terrified, and though they were not financially stable, she somehow managed to get the surgery done. She remembers the surgeon saying, “Little girls should not have testicles”. Her gonads were removed and was put on hormonal replacement therapy.
The revelation
The endocrinologist had done a karyotype test on her, which revealed she was 46, XY, a result she only became aware of by chance when she was 26 years old. She had tripped on a box filled with her mother’s stuff. She saw the karyotype result and was so confused, that it said: “A discrepancy between the genotype (XY) and the reported phenotype (female) is noted.”
She called her cousin who was a medical professional. Her cousin, who already knew about her condition, explained what androgen insensitivity syndrome was to her and was surprised she did not know about her diagnosis.
She was dumbfounded and felt cheated after getting to know the truth about her condition, as her family somewhat knew, but no one told her. She was never properly counselled and or given a clear explanation of her condition.
She was placed on Hormonal Replacement Therapy (HRT), Premarin. At 18, she could no longer continue getting the HRT, as she could not afford it. Here she was in her twenties sexually naïve, just knowing about her own reality. She grew up in a sex-shaming, purity culture, and she avoids sex and dating.
She had a lot of questions about where to go, and what to do about her condition, but was sceptical about seeing an OBGYN because she absolutely did not want a pelvic exam, especially remembering her traumatising first visit.
The awkwardness and unempathetic medical professionals
She told us of one occasion when she summoned the courage to see one doctor, who said during the consultation, “Do you mind me going to get my interns I want to educate them, we have only read of this condition in the textbooks.” She said, “Okay but immediately took her bag, left the hospital, and never returned.”
She experienced hot flashes, sexual difficulties, mood swings, and temperature dysregulation as she was not under HRTs. At 26 she was able to gather the courage to see a primary care physician and ask for a pelvic exam. The doctor, who personally knew her, referred her to another physician.
The new doctor was kind, very understanding, and explained things to her as he was doing them. After the examination, he explained to her that everything was alright with her genitals. She was a bit embarrassed, but relieved because she knew she was “functional”.
For a long time, she was not able to go back on treatment because doctors refused to see her, saying she had to see an endocrinologist, stating that she was not a “normal” woman. Endocrinologists denied giving her treatment, saying it was not medically necessary.
At 37, she was able to get the HRT medicine as she could afford finally. She states that 20 years without HRT was “really a lot to handle”. She revealed that when people find out she is intersex, they say things like ‘I always knew something was different’, because of her physique. She states that while a masculine physique may be part of the signs of androgen insensitivity syndrome, it is not always the case and was not in her case.
Her heart-touching story helped us to see the real struggles of people with androgen insensitivity syndrome especially as regards their relationship with family, friends, and physicians. Her story highlights the importance of counselling and the impact on mental health in people with androgen insensitivity syndrome.
It also highlights some potholes in the management of patients with androgen insensitivity syndrome, such as immediate removal of gonads at diagnosis, and needless pelvic examinations for the sake of “standard procedures”, and shows the need for individualised management.
Her story focuses on ensuring that androgen insensitivity syndrome patients understand their condition fully, and encourages doctors to treat them with empathy, not as a science experiment.